
Menopause and Mental Health
By 2050, women over 50 will make up about 23% of the US population. Considering that the average age of menopause is 51 for western women, the majority of that 23% will be menopausal or post menopausal.
Wherever you are in life, having an understanding of the state of your body, what your ‘normal is,’ and the changes to come is incredibly important. Women are particularly sensitive to hormonal shifts, and the post menopausal years bring falling levels of estrogen and emotional and physical changes.
Many women come to major hormonal milestones of menopause, with relatively little preparation or understanding of the hormonal shift that are about to take place. While we may know about the falling estrogen levels, cessation of the monthly period, possible weight gain, and hot flashes, most of us are not aware of the various emotional changes that go along with the hormone changes. Did you know that women in post menopausal years are at an increased risk for depression and anxiety? Your ovaries produce less estrogen which in turn affects the levels of serotonin in your brain. And estrogen’s role in serotonin production is just one of the many important roles it plays in women’s mental health.
If you are one of the 25 million women around the world going through menopause right now, this article is for you. It’s also for any post- menopausal woman experiencing a new hormonal landscape, and it’s for all the pre and perimenopausal women seeking a better understanding of the hormonal journey ahead. We’re discussing the impact that a drop in estrogen has on women in post menopause, and the treatments available for those suffering from hormonal changes, and who need support traversing the new hormonal landscape.
Welcome to Menopause
Women in the US will ovulate over 400 times in the course of a lifetime. This is more than at any other period in history, and more than women in the southern part of the world, who will get their period only about 70 times. Apart from having fewer children, western women are also getting their periods earlier thanks in large part to xenoestrogens in our environment.
Women are born with about 1-2 million eggs, a number that drops to about 300,000 to 400,00 at puberty, and then about 1,000 eggs die each month. The reason that the onset of menopause differs between women is because we get to our last viable eggs at different times, depending on how many eggs we had going into puberty.
By 35 years old, 60% of a woman’s eggs are ripe and ready to go. By age 45 that number has dropped to just 15%. As you start to “run low on eggs,” your ovaries and brain will detect the change and trigger the production of more FSH or follicle stimulating hormone - the hormone that helps to mature and produce eggs from the ovaries. This FSH increase will lead to increased estrogen, which can increase heaviness of flow and exacerbate estrogen related physical and emotional symptoms.
In the late reproductive stages, the menstrual cycle may become shorter in length and frequency. Eventually cycles become increasingly varied in length, and once they vary by 7 days you’ve officially hit menopause or late stage perimenopause. By this point, the egg follicles that the FSH is trying to pump out are all but gone, and the body stops producing estrogen at the high levels it once did. As follicles continue to decrease in number, there is a decrease in ovulation and progesterone production resulting in lighter and more infrequent bleeding with 35 plus days between cycles. The time between periods grows longer, and eventually, around 51 (range is 45 to 55) years old, the final menstrual period (FMP) flows. After this, there is very little estrogen being produced, and after one year of no menstruation, post- menopause life begins.
Estrogen after Menopause
For many women, life after monthly periods (not to mention the cramps, dirty sheets, ruined underwear, and missed productivity that goes along with it) is embraced with open arms. Lower, consistent levels of estrogen often mean increased emotional stability as well.
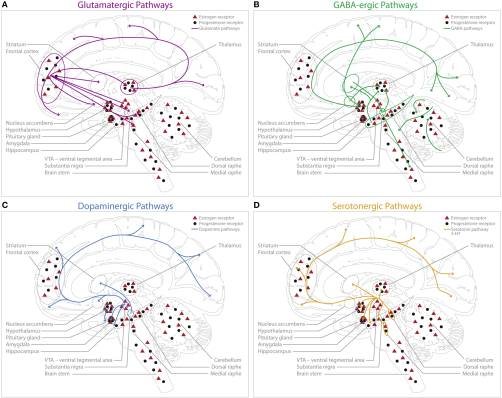
The different neural pathways affected by estrogen! Don’t feel like you have to understand the specifics of these pathways and how estrogen is involved- scientists are still figuring this out. Instead, I am including this just to emphasize the innumerable ways that estrogen impacts women’s brains.
Source: Barth et Al, 2015. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4335177/#!po=2.35849
For many women though, life after menopause can be challenging as the body adjusts to chronically low levels of a hormone that once kept you energized, lubricated, and happy. Estrogen plays over 300 roles in the female body, and you may be surprised to learn that many of those are in the brain.
Estrogen has been found to be highly active in the areas of the brain involved in cognition and emotion such as the amygdala and hippocampus. Together with progesterone, estrogen may act as a critical neuroregulatory, neurotropic, and neuroprotective agent in brain physiology and disease states. Estrogen can act not only via estrogen specific receptors in the brain, but also via other receptor types including those for serotonin and dopamine.
Estrogen and progesterone have been found to affect brain neurotrophic factor (BDNF), which is involved in the growth, survival, and proliferation of brain cells. After brain injury, BDNF supports neuronal regeneration and helps regulate neurotransmitters. Studies show that hormone replacement treatment increases BDNF in the hippocampus, amygdala, and prefrontal cortex of the brain. Unsurprisingly, menopause and chronically low levels of estrogen are characterized by an increased risk for diseases like Parkinson’s and Alzheimers.
We mentioned that estrogen can use the receptors in the brain meant for neurotransmitters like dopamine and serotonin, and it can do this in two ways: by altering the ability of a neuron to release neurotransmitters in the first place (like dopamine and serotonin), and by altering the responsiveness of neighboring neurons to “retrieve” neurotransmitters that have been released.
Women after menopause are at high risk for conditions involving the Dopamine transporter (DAT) pathways. DAT is responsible for taking in excess dopamine and is related diseases include Parkinson’s, ADHD, Tourettes, and Alzheimers. We are also at increased risk for other behavioral health disorders including depression, anxiety, ADHD, insomnia, and disorders involving the brain’s reward circuits including addiction.
“A woman's lifespan is characterized by major hormonal transition periods beginning with rising estrogen level during puberty (Angold et al., 1998), high estrogen levels during pregnancy and rapid falls postpartum (Galea et al., 2001), declining levels during perimenopause (Cohen et al., 2006a) and low levels postmenopausal. Intriguingly, these major shifts in sex hormone levels seem to be paralleled by the incidence rates of mood disorders such as unipolar depression (Figure 2). According to the monoamine hypotheses of depression (Hindmarch, 2002), depressed mood seems to be accompanied by alternations in neurotransmitter functioning and transmission. Ovarian hormones are known to exhibit modulatory effects on synaptic transmission. These modulatory effects can be achieved by altering the responsiveness of postsynaptic receptors (Yankova et al., 2001; Maejima et al., 2013) or the presynaptic release of neurotransmitters (Yokomaku et al., 2003). The alternation of both mechanisms largely affect the neurochemical systems involved in healthy emotional and cognitive control, such as dopaminergic, serotonergic, glutamatergic and γ-aminobutyric acid (GABA)-ergic systems.”
What this all means is that estrogen plays a major role in women’s brain health, and chronically low estrogen levels after menopause can mean significant emotional and physical shifts. Whether or not to treat low hormone levels is still under debate and will likely depend on the severity of your symptoms.
Effect of Low Estrogen Levels
Low levels of estrogen during menopause can negatively impact some of the most important areas in a woman’s life according a gynecologist Dr. Gottfried (author of Hormone Cure): sex, appetite, weight, sleep, and fertility. Estrogen helps innervate genital skin and keep it well supplied with blood flow and lubrication. Low levels can lead to vaginal dryness, more subtle orgasms, and sex that seems to “take more effort.” Lower levels of serotonin are likely to set in which can lead to depression or erratic moods. And thermoregulation of the body becomes unpredictable as estrogen levels decline.
After menopause, it isn’t just that your estrogen levels drop that puts you at risk for unpleasant side effects including depression and anxiety, it’s that your estrogen may become out of balance with another very important sex hormone: progesterone. According to Dr. Sara Gottfried, estrogen and progesterone must be in balance as they operate like two parts to a whole, yin and yang. For example estrogen is known to be associated with water and salt retention while progesterone is a natural diuretic. Estrogen stimulates cell growth in breast tissue while progesterone helps prevent too much cell growth that can lead to painful cysts. When in balance, progesterone and estrogen help maintain strong, dense bones; hydrated and smooth skin; a healthy metabolism; and a cardiovascular system free from blood clots and plaque buildup.
Lower estrogen levels can result in vasomotor symptoms, present in 40% of perimenopausal women directly before menopause and 85% of post-menopausal women.
Other symptoms of low estrogen include:
heart palpitations
headaches
dizziness
mood variability
attention and memory disorders
despondency
anxiety
depression
Hot flushes and night sweats– related to fluctuations in estrogen – sweating, heart palpitations, anxiety and flushing, can trigger poor sleep and psychological and physical consequences of poor sleep.
vaginal dryness and atrophy
weight gain
bone loss
increased risk of heart disease
skin dryness and wrinkles
increased risk for bladder infections
sleep disruption
Treatment of Low Estrogen
If you are post menopausal and checking off multiple symptoms on the list above, you may consider getting a blood test to check your hormone levels. As science is still discovering all of the very important roles that hormones play, it is common for doctors to dismiss the idea of hormone testing as wasteful or inefficient, but the truth is that it is as valuable to track and compare your hormone levels for your own health and understanding of where you are in the hormone change process. There are saliva, urine, and blood tests available to test estrogen levels in the body, though there is some confusion over which method is best, and even debate as to the optimal levels of estrogen for post-menopausal women.
The hormone changes of menopause are a natural process and not an illness and for most women no treatment is needed.
It is also important to note that it is still contested whether and for how long low estrogen levels need to be addressed in post-menopausal women. Low levels of estrogen is not an inherently bad thing. Studies have shown that vegetarians have lower estrogen levels and lower lifetime rates of breast cancer. Similarly, Japanese women tend to eat more soy and less meat and have a 5 fold decreased risk for breast cancer than women in the US. Japanese women also tend to eat less fat and more fiber, with the latter helping to excrete used up estrogen from the body. It is always best to consult with your healthcare provider, and if possible, with an integrative healthcare professional, in order to best understand where your hormone levels are and what treatment may be best for you.
Lifestyle and dietary changes should be adopted before any more intensive therapy is pursued. Hormone replacement therapy (HRT), phytoestrogens (naturally occurring in plants), and anti-depressant medications are also all used successfully to treat low estrogen and the side effects that it causes. However, the latter three treatments come with a range of side effects, particularly HRT and antidepressant pharmacotherapy, and should again only be adopted when lifestyle and diet interventions are unsuccessful.
The good news is that the following lifestyle and dietary changes can really go a long way towards balancing estrogen levels and making you feel your best. See Dr. Gottfried’s book for additional information.
Lifestyle, Herbs, and Nutraceuticals
Avoid coffee/ caffeine
Eat more whole unprocessed and organic soy
Cut out gluten
Add flaxseed to your meals
Ghee — for vaginal dryness
Pomegranate
Vitamin E
Magnesium
Maca
Rhubarb
St. john’s wort + black cohosh — believed to alleviate menopause related emotional disorders like anxiety and depression
Ginseng — for memory
Hops
Valerian root — for sleep
Gabapentin — decreases hot flushes
Relaxation exercises
Hypnosis
Mindfulness
Cognitive Behavioral Therapy
Spiritual and existential exploration and positive attitude towards the transition
Orgasm more — help with blood flow and relaxation
Acupuncture — effective once or twice a week
Yoga — helps for psychological side effects
Don’t exercise too much-can cause high cortisol levels
Hormone Therapy, Phytoestrogens, and Antidepressants
If the above interventions do not provide relief, talk to your doctor about treatment with phytoestrogens, hormone replacement therapy (HRT) and/or antidepressant therapy. HRT with estrogen will help to raise serotonin which will likely improve mood, sleep, appetite, and sex drive according to Dr. Gottfried. Estrogen therapy will help with the emotional and physical depressive and/or anxiety problems you may be experiencing. The drawback is that hormone replacement therapy comes with side effects, and this is the reason doctors are likely to pushback against it, if they even provide it at all. If you have a history of fibroids or blood clots in the leg or lungs, if you have undiagnosed vaginal bleeding, active gall bladder disease, or liver disease you should not consider HRT. Taking estrogen can worsen symptoms in some cases. However, despite the possible risks, many women find relief using HRT. Estradiol patches are FDA approved and considered safe when used appropriately. Estrogen needs to be used in combination with progesterone to protect from breast cancer and other risks of unopposed estrogen.
Phytoestrogens are naturally occurring estrogen variants found in plants. Asian diets are high in phytoestrogen, containing 10 times as much as the standard American diet. As noted earlier, Asian women have lower rates of breast cancer and less dramatic symptoms of menopause like hot flashes, osteoporosis, and worsening heart disease. More study is needed to really understand the full benefits and cost of phytoestrogen therapy, but it has been shown to lower the risk of estrogen related cancers and it may protect against brain damage, but further study is needed.
In regards to HRT, a good rule of thumb is to design a regimen that delivers the most effective estrogens, at lowest possible effective doses, with most effective scheduling, and fewest side effects. Due to the complicated mechanisms of action in the body, HRT should only be undertaken with care and expert guidance. The dose, specific metabolites, co-HRT with progesterone, timing, and duration of treatment should be individualized.
Here are some of the potential risks associated with longterm use of HRT based on Women’s Health Initiative (WHI) studies:
potential increase risk for cancer of the breast, uterus, endometrium
increase of dense breast tissue and difficulty with accurate mammography
potential exacerbation of cardiovascular problems
more study is needed on other possible effects such as possible decline in cognitive functioning
Antidepressant medications are also a common treatment option for women experiencing depression or anxiety during the post menopause years. Selective serotonin reuptake inhibitors (SSRIs) and serotonin and norepinephrine reuptake inhibitors (SNSRIs) can help with hot flashes and mood symptoms post menopause.
In a recent study, “Conventional or Natural Pharmacotherapy and the Prevalence of Anxiety and Depression During Menopause,” researchers compared the effectiveness of several types of pharmacotherapy: phytoestrogen therapy, HRT, anti-depressant therapy, or a combination of HRT + anti-depressant therapy in women with anxiety and/ or depression across the lifespan. A total of 795 women completed the study surveys which measured (1) the severity of menopausal symptoms, (2) the severity of anxiety and depression disorders, (3) the general state of mental health, and (4) participants’ belief in the effectiveness of their own pharmacotherapy regimen.
Researchers found that the presence and severity of symptoms associated with hormonal shifts were most prominent in the perimenopausal period and in the first 2 years post menopause, with declining levels thereafter. They also found that depression and anxiety symptoms were more severe during the perimenopause years, but do note that there have been previous studies showing a direct link between menopause and depression.
A few interesting trends that the researchers also found:
In the 1-2 years on either side of menopause, women are increasingly beginning treatment for emotional disorders
HRT used to treat emotional disorders had following positive outcomes:
improves participants quality of life by removing vasomotor symptoms
enhances effects of antidepressants and mood in some women
women report high rates of satisfaction with this therapy
Women who used HRT for less than 2 years reported higher satisfaction with its efficacy than women who used it for over 2 years
this has been corroborated by other studies that indicate HRT benefit may peak around 2-5 years and then may lead to adverse side effects
The greater the severity of menopausal symptoms, the poorer the woman’s evaluation of her mental health
Women who were not undergoing treatment with SSRIs or SNRIs had more severe, frequent anxiety symptoms and were at greater risk for depression
Researchers concluded that phytoestrogen therapy was the best method of treatment with the smallest risk for side effects, and with the highest perceived patient satisfaction. They noted that one major benefit of this type of therapy is that it does not require chronic use of antidepressants or HRT and thus has fewer side effects. Its efficacy depended on lifestyle, dosage, and duration of use and again, it was mostly used in women with perimenopause, so more study is needed to see if this treatment is as effective for post-menopausal women. The researchers noted that treatment with HRT alone or with HRT + SSRI or SNRI combination therapy was effective but has more side effects. HRT can cause frequent mood swings, so women should proceed with caution when using this option.
Conclusion and Recommendations
Life after menopause can be a time of increased emotional stability without the disruption of a monthly period. Yet, shifts in our hormonal landscape can cause post menopausal women to become anxious, depressed. Lifestyle interventions along with more aggressive HRT, phytoestrogen, and antidepressant therapies are available to women who are looking for relief.
Dr. Beata Lewis of Mind Body Seven works with women in peri-menopause and menopause to address the mental health impact of hormone shifts. Dr. Lewis can monitor hormone levels through bloodwork and address peri-menopause symptoms with lifestyle based approaches for balancing hormones. As Dr. Sara Gottfried says, the post- menopausal years do not have to be dry and boring, they can be juicy and exhilarating. And after 400+ periods in one lifetime, I think we deserve at least that much.